Targets: To examine the amount/level of Physical Activity (PA) needed to generate the most health benefits in noninstitutionalized 75 year and older U.S. resident adults. Intervention description: A total of 598 sample participants aged 75 year and above from National Health And Nutrition Examination Survey (NHANES) 2005-2006 datasets were included. Actigraph-monitored daily step counts, self-reported PA duration (time spent in weekly PA) and weekly energy expenditure were used to describe PA level/amount. Functional ability was expressed using the total levels of difficulties in doing twenty-one types of daily activities. PRISM Dose-response Curves Stimulation Variable slope model was applied to examine the needed PA level/amount in the population. Mechanisms of action: PA benefits functional health in 75 year and older adults. Older females aged 75- 84 year need at least 150 mins/ 800 kcal energy expenditure per week or 5,800 daily steps to reach the most functional benefits. Older men aged 75-84 year need walk about 5,800 steps/day to achieve higher level of functionality. Older adults aged 85 years and above need to spend about 240 minutes/week on PA to gain health benefits. Outcomes: Older males generally need/engage in more amount of PA compared to their female counterparts. Between 75-84 year old male and female adults, PA intensity is more important/reflective in male for expressing PA amount, while time spent in PA is more meaningful to older females. There is no difference in needed PA amount between different genders in 85 year and older adults.
| Published in | Science Journal of Public Health (Volume 12, Issue 3) |
| DOI | 10.11648/j.sjph.20241203.15 |
| Page(s) | 92-102 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Physical Activity, Older Adults, Functional Ability, Walking Steps, Energy Expenditure, Dose-Response
Percent/Mean SD (Middle-old) | Percent/Mean SD (Old-old) | |
|---|---|---|
Sample Size | N=428 | N=170 |
Age | 79.52.80 | 85 |
Gender | ||
Male | 236 (55.1%) | 65 (38.2%) |
Female | 192 (44.9%) | 105 (61.8%) |
Marital Status | ||
Married | 230 (53.7%) | 43 (25%) |
Widowed | 144 (33.6%) | 117 (68.8%) |
Divorced | 37 (8.6%) | 1 (0.6%) |
Separated | 7 (1.6%) | 2 (1.2%) |
Never married | 7 (1.6%) | 3 (1.8%) |
Race/Ethnicity | ||
Non-Hispanic White | 324 (75.7%) | 137 (80.6%) |
Non-Hispanic Black | 60 (14%) | 17 (10%) |
Mexican American | 31 (7.2%) | 11 (6.5%) |
Other Race -including multi-racial | 8 (1.9%) | 5 (2.9%) |
Other Hispanic | 5 (1.2%) | 0 (0%) |
Education Level | ||
Less Than 9th Grade | 94 (22%) | 45 (26.5%) |
9-11th Grade(Includes 12th grade with no diploma) | 70 (16.4%) | 26 (15.3%) |
High School Grad/GED or Equivalent | 118 (27.6%) | 41 (24.1%) |
Some College or AA degree | 92 (21.5%) | 39 (22.9%) |
College Graduate or above | 52 (12.1%) | 16 (9.4%) |
Total Numbers of Medical Conditions | ||
Zero medical condition | 91 (21.3%) | 21 (12.4%) |
1-2 medical conditions | 206 (48.1%) | 101 (59.4%) |
3-5 medical conditions | 111 (26%) | 43 (25.2%) |
>5 medical conditions | 19 (4.4%) | 5 (3%) |
Body Mass Index (BMI) | 27.35.17 | 25.64.47 |
n | Difficulty level in doing 20 types of daily activities (Mean SD) | n | Steps per day (Mean SD) | n | Weekly energy expenditure (kcal) (Mean SD) | n | Weekly PA duration (min) (Mean SD) | |
|---|---|---|---|---|---|---|---|---|
Middle-old | ||||||||
Male | 142 | 22.64.12 | 202 | 53823009 | 169 | 29293705<sup></sup> | 178 | 479616<sup></sup> |
Female | 106 | 24.36.44<sup></sup> | 157 | 48102691 | 104 | 17072519 | 115 | 342445 |
Total | 248 | 23.3 5.29 | 359 | 51322884 | 273 | 24643352 | 293 | 425558 |
Old-old | ||||||||
Male | 30 | 25.56.73 | 46 | 42033750 | 34 | 18292158<sup></sup> | 40 | 332381 |
Female | 25 | 27.89.82 | 69 | 28062354 | 37 | 9571205 | 37 | 227275 |
Total | 55 | 26.5 8.28<sup></sup> | 115 | 33653054 | 71 | 13751771 | 77 | 282336 |
Middle-old female | Middle-old male | Male old-old | Female old-old | |
|---|---|---|---|---|
Best-fit values | ||||
Bottom | -22.02 | -22.23 | -24.64 | -24.15 |
Top | -29.46 | Unstable | -22.60 | -23.25 |
logEC50 | 61.91 | Unstable | Unstable | Unstable |
HillSlope | -0.02378 | Unstable | Unstable | Unstable |
EC50 | 8.190e+061 | Unstable | Unstable | Unstable |
Span | -7.434 | Unstable | 2.041 | 0.8998 |
95% CI (profile likelihood) | ||||
Bottom | -23.59 to -20.29 | -22.90 to -21.55 | -29.58 to -21.82 | -27.45 to-22.55 |
Top | ? | (very wide) | -26.48 to -18.72 | -25.84 to-20.66 |
Goodness of Fit | ||||
Degrees of Freedom | 69 | 120 | 16 | 30 |
R squared | 0.2211 | 0.000 | 0.06906 | 0.01852 |
Sum of Squares | 1022 | 1748 | 495.8 | 680.1 |
Sy.x | 3.848 | 3.816 | 5.566 | 4.761 |
Number of points | ||||
# of X values | 293 | 176 | 40 | 77 |
# Y values analyzed | 73 | 124 | 20 | 34 |
Middle-old | |
|---|---|
Best-fit values | |
Bottom | -22.79 |
Top | -23.84 |
Span | -1.044 |
95% CI (profile likelihood) | |
Bottom | -23.68 to -21.90 |
Top | -24.76 to -22.92 |
Goodness of Fit | |
Degrees of Freedom | 211 |
R squared | 0.01206 |
Sum of Squares | 4792 |
Sy.x | 4.766 |
Number of points | |
# of X values | 876 |
# Y values analyzed | 215 |
Middle-old | Female middle-old | |
|---|---|---|
Best-fit values | ||
Bottom | -22.75 | -22 |
Top | -21.50 | -24.16 |
Span | 1.255 | -2.161 |
95% CI (profile likelihood) | ||
Bottom | -23.39 to -22.12 | -23.39 to -20.61 |
Top | -22.88 to -20.12 | -25.64 to -22.69 |
Goodness of Fit | ||
Degrees of Freedom | 179 | 62 |
R squared | 0.01456 | 0.06838 |
Sum of Squares | 2814 | 1046 |
Sy.x | 3.965 | 4.108 |
Number of points | ||
# of X values | 714 | 273 |
# Y values analyzed | 183 | 66 |
PA | Physical Activity |
NHANES | National Health and Nutrition Examination Survey |
PAGAC | Physical Activity Guidelines Advisory Committee |
NCHS | National Center for Health Statistics |
HHS | Department of Health and Human Services |
PFQ | Physical Functioning Questionnaires |
PAQ | Physical Activity Questionnaires |
| [1] | Zizza, C. A., Ellison, K. J., & Wernette, C. M. (2009). Total Water Intakes of Community- Living Middle-Old and Oldest-Old Adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 64A (4): 481–486. |
| [2] | Little, W., & McGivern, R. (2019). Aging and the Elderly. Introduction To Sociology- 1st Canadian Edition. licensed under a Creative Commons Attribution 4.0 International License. |
| [3] | Cicirelli, Victor G. (2002). Older Adults' Views on Death. Springer Pub. ISBN 9780826170125. |
| [4] |
Jacelon C. S. (2010). Maintaining the balance: older adults with chronic health problems manage life in the community. Rehabilitation nursing : the official journal of the Association of Rehabilitation Nurses, 35(1), 16–40.
https://doi-org.silk.library.umass.edu/10.1002/j.2048-7940.2010.tb00026.x |
| [5] | U.S. Department of Health and Human Services. (2018). Physical Activity Guidelines for Americans, 2nd edition. Washington, DC: U.S. Department of Health and Human Services. |
| [6] | World Health Organization. (2020). Guidelines on Physical Activity and Sedentary Behaviour. Geneva: World Health Organization; License: CC BY-NC-SA 3.0 IGO. |
| [7] | Sun, F., Norman, I. J., & While, A. E. (2013). Physical activity in older people: A systematic review. BMC Public Health, 13, 449. |
| [8] | Bouchard, C., W. Hollmann, H. Venrath, G. Herkenrath, & H. Schlussel. (1966). Minimal amount of exercise for the prevention of cardiovascular diseases (Minimalbelastungen zur Pra¨vention Kardiovaskularer Erkrankungen). Sportarzt und Sportmedizin. 17: 348–357. |
| [9] | Bouchard, C. (2001). Physical activity and health: Introduction to the dose-response symposium. Medicine and Science in Sports and Exercise, 33(6 Suppl), S347-350. |
| [10] | Antero Kesaniemi, Y., Danforth, E., Jensen, M. D., Kopelman, P. G., Lefèbvre, P., & Reeder, B. A. (2001). Dose-response issues concerning physical activity and health: An evidence-based symposium. Medicine & Science in Sports & Exercise, 33(6), S351. |
| [11] | Etman, A., Pierik, F. H., Kamphuis, C. B. M., Burdorf, A., & van Lenthe, F. J. (2016). The role of high-intensity physical exercise in the prevention of disability among community-dwelling older people. BMC Geriatrics, 16(1), 183. |
| [12] | Pereira, C., Baptista, F., & Cruz-Ferreira, A. (2016). Role of physical activity, physical fitness, and chronic health conditions on the physical independence of community-dwelling older adults over a 5-year period. Archives of Gerontology and Geriatrics, 65, 45–53. |
| [13] | Fielding, R. A., Guralnik, J. M., King, A. C., Pahor, M., McDermott, M. M., Tudor-Locke, C., Manini, T. M., Glynn, N. W., Marsh, A. P., Axtell, R. S., Hsu, F.-C., & Rejeski, W. J. (2017). Dose of physical activity, physical functioning and disability risk in mobility-limited older adults: Results from the LIFE study randomized trial. Plos One, 12(8), e0182155. |
| [14] | Tomita, M. R., Fisher, N. M., Nair, S., Ramsey, D., & Persons, K. (2018). Impact of Physical Activities on Frailty in Community-Dwelling Older Women. Physical & Occupational Therapy in Geriatrics, 36(1), 107–119. |
| [15] | Physical Activity Guidelines Advisory Committee. (2018) 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services. |
| [16] | Cabanas-Sánchez, V., Higueras-Fresnillo, S., De La Cámara, M. Á., Esteban-Cornejo, I., & MARTÍNEZ-GÓmez, D. (2019). 24-h Movement and Nonmovement Behaviors in Older Adults. The IMPACT65+ Study: Medicine & Science in Sports & Exercise, 51(4), 671–680. |
| [17] | Tudor-Locke, C., Hatano, Y., Pangrazi, R. P., & Kang, M. (2008). Revisiting “How Many Steps Are Enough?”: Medicine & Science in Sports & Exercise, 40(Supplement), S537–S543. |
| [18] | Tudor-Locke Catrine, Craig Cora L, Aoyagi Yukitoshi, Bell Rhonda C, Croteau Karen A, De Bourdeaudhuij Ilse, Ewald Ben, Gardner Andrew W, Hatano Yoshiro, Lutes Lesley D, Matsudo Sandra M, Ramirez-Marrero Farah A, Rogers Laura Q, Rowe David A, Schmidt Michael D, Tully Mark A, & Blair Steven N. (2011). How many steps/day are enough? For older adults and special populations. International Journal of Behavioral Nutrition and Physical Activity, 1, 80. |
| [19] | Tudor-Locke, C., & Bassett, D. R. (2004). How Many Steps/Day Are Enough?: Preliminary Pedometer Indices for Public Health. Sports Medicine, 34(1), 1–8. |
| [20] | Kang, M., Marshall, S. J., Barreira, T. V., & Lee, J.-O. (2009). Effect of Pedometer-Based Physical Activity Interventions: A Meta-Analysis. Research Quarterly for Exercise & Sport, 80(3), 648–655. |
| [21] | Kraus, W. E., Janz, K. F., Powell, K. E., Campbell, W. W., Jakicic, J. M., Troiano, R. P., Sprow, K., Torres, A., & Piercy, K. L. (2019). Daily Step Counts for Measuring Physical Activity Exposure and Its Relation to Health: Medicine & Science in Sports & Exercise, 51(6), 1206–1212. |
| [22] | Aoyagi, Y., Park, H., Watanabe, E., Park, S., & Shephard, R. J. (2009). Habitual physical activity and physical fitness in older Japanese adults: The Nakanojo Study. Gerontology, 55(5), 523–531. |
| [23] | de Melo, L. L., Menec, V. H., & Ready, A. E. (2014). Relationship of functional fitness with daily steps in community-dwelling older adults. Journal of Geriatric Physical Therapy (2001), 37(3), 116–120. |
| [24] | Ewald, B., Attia, J., & McElduff, P. (2014). How Many Steps Are Enough? Dose--Response Curves for Pedometer Steps and Multiple Health Markers in a Community-Based Sample of Older Australians. Journal of Physical Activity & Health, 11(3), 509–518. |
| [25] | Havighurst, R. J. (1961). "Successful ageing". The Gerontologist. 1: 8– 13. |
| [26] | Haskell, W. L. (1994). Health consequences of physical activity: under Standing and challenges regarding dose-response. Med. Sci. Sports Exer, 26: 649–660. |
| [27] | Haskell, W. L. (1994). Dose-response issues from a biological perspective. In: Physical Activity, Fitness, and Health, C. Bouchard, R. J. Shephard, and T. Stephens (Eds.). Champaign, IL: Human Kinetics, pp. 1030–1039. |
| [28] | Shephard, R. J. (2002). Gender, physical activity, and aging. CRC Press. |
| [29] | Spirduso, W. W. & Cronin, D. L. (2001). Exercise dose-response effects on quality of life and independent living in older adults. Med Sci Sports Exerc. 33: S598-608; discussion S609-510, 2001., DC, 2005. |
| [30] | Rankinen, T., Bouchard, C., Corbin, C. B., Pangrazi, R. P., & Franks, D. (2002). Dose-Response Issues Concerning the Relations Between Regular Physical Activity and Health [dataset]. American Psychological Association. |
| [31] | Anderssen, S. A., & Strømme, S. B. (2001). Physical activity and health—Recommendations. Tidsskrift for den Norske laegeforening, 121(17), 2037–2041. |
| [32] | Sparling, P. B., Howard, B. J., Dunstan, D. W., & Owen, N. (2015). Recommendations for physical activity in older adults. BMJ: British Medical Journal, 350. |
| [33] | Manini, T. M., & Pahor, M. (2009). Physical activity and maintaining physical function in older adults. British Journal of Sports Medicine, 43(1), 28–31. |
| [34] | Lopes de Pontes, T., Pinheiro Amador Dos Santos Pessanha, F., & Freire, R. C., et al. (2021). Total Energy Expenditure and Functional Status in Older Adults: A Doubly Labelled Water Study. J Nutr Health Aging, 25, 201–208. |
| [35] | Hall, K. S., Morey, M. C., Dutta, C., Manini, T. M., Weltman, A. L., Nelson, M. E., Morgan, A. L., Senior, J. G., Seyffarth, C., & Buchner, D. M. (2014). Activity-Related Energy Expenditure in Older Adults: A Call for More Research. Medicine & Science in Sports & Exercise, 46(12), 2335–2340. |
| [36] | Sarling, R. D. (2001). Energy Expenditure and Aging: Effects of Physical Activity. International Journal of Sport Nutrition and Exercise Metabolism, 11, S208-S217. |
| [37] | Dondzila, C. J. 1, cdondzil@citadel. edu, Gennuso, K. P. 2, Swartz, A. M. 2, Tarima, S., Lenz, E. K. 4, Stein, S. S. 5, Kohl, R. J. 5, & Strath, S. J. 2. (2015). Dose-Response Walking Activity and Physical Function in Older Adults. Journal of Aging & Physical Activity, 23(2), 194–199. |
| [38] | Duncan, M., Minatto, G., & Leddington wright, S. (2016). Dose-response between pedometer assessed physical activity, functional fitness, and fatness in healthy adults aged 50-80 years: DOSE-RESPONSE OF PHYSICAL ACTIVITY. American Journal of Human Biology, 28. |
APA Style
Chen, C., Jacelon, C., Choi, J. (2024). How Much Physical Activity Is Needed for 75 Year and Older Adults: Using NHANES Datasets. Science Journal of Public Health, 12(3), 92-102. https://doi.org/10.11648/j.sjph.20241203.15
ACS Style
Chen, C.; Jacelon, C.; Choi, J. How Much Physical Activity Is Needed for 75 Year and Older Adults: Using NHANES Datasets. Sci. J. Public Health 2024, 12(3), 92-102. doi: 10.11648/j.sjph.20241203.15
@article{10.11648/j.sjph.20241203.15,
author = {Chunfang Chen and Cynthia Jacelon and Jeungok Choi},
title = {How Much Physical Activity Is Needed for 75 Year and Older Adults: Using NHANES Datasets
},
journal = {Science Journal of Public Health},
volume = {12},
number = {3},
pages = {92-102},
doi = {10.11648/j.sjph.20241203.15},
url = {https://doi.org/10.11648/j.sjph.20241203.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20241203.15},
abstract = {Targets: To examine the amount/level of Physical Activity (PA) needed to generate the most health benefits in noninstitutionalized 75 year and older U.S. resident adults. Intervention description: A total of 598 sample participants aged 75 year and above from National Health And Nutrition Examination Survey (NHANES) 2005-2006 datasets were included. Actigraph-monitored daily step counts, self-reported PA duration (time spent in weekly PA) and weekly energy expenditure were used to describe PA level/amount. Functional ability was expressed using the total levels of difficulties in doing twenty-one types of daily activities. PRISM Dose-response Curves Stimulation Variable slope model was applied to examine the needed PA level/amount in the population. Mechanisms of action: PA benefits functional health in 75 year and older adults. Older females aged 75- 84 year need at least 150 mins/ 800 kcal energy expenditure per week or 5,800 daily steps to reach the most functional benefits. Older men aged 75-84 year need walk about 5,800 steps/day to achieve higher level of functionality. Older adults aged 85 years and above need to spend about 240 minutes/week on PA to gain health benefits. Outcomes: Older males generally need/engage in more amount of PA compared to their female counterparts. Between 75-84 year old male and female adults, PA intensity is more important/reflective in male for expressing PA amount, while time spent in PA is more meaningful to older females. There is no difference in needed PA amount between different genders in 85 year and older adults.
},
year = {2024}
}
TY - JOUR T1 - How Much Physical Activity Is Needed for 75 Year and Older Adults: Using NHANES Datasets AU - Chunfang Chen AU - Cynthia Jacelon AU - Jeungok Choi Y1 - 2024/06/26 PY - 2024 N1 - https://doi.org/10.11648/j.sjph.20241203.15 DO - 10.11648/j.sjph.20241203.15 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 92 EP - 102 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20241203.15 AB - Targets: To examine the amount/level of Physical Activity (PA) needed to generate the most health benefits in noninstitutionalized 75 year and older U.S. resident adults. Intervention description: A total of 598 sample participants aged 75 year and above from National Health And Nutrition Examination Survey (NHANES) 2005-2006 datasets were included. Actigraph-monitored daily step counts, self-reported PA duration (time spent in weekly PA) and weekly energy expenditure were used to describe PA level/amount. Functional ability was expressed using the total levels of difficulties in doing twenty-one types of daily activities. PRISM Dose-response Curves Stimulation Variable slope model was applied to examine the needed PA level/amount in the population. Mechanisms of action: PA benefits functional health in 75 year and older adults. Older females aged 75- 84 year need at least 150 mins/ 800 kcal energy expenditure per week or 5,800 daily steps to reach the most functional benefits. Older men aged 75-84 year need walk about 5,800 steps/day to achieve higher level of functionality. Older adults aged 85 years and above need to spend about 240 minutes/week on PA to gain health benefits. Outcomes: Older males generally need/engage in more amount of PA compared to their female counterparts. Between 75-84 year old male and female adults, PA intensity is more important/reflective in male for expressing PA amount, while time spent in PA is more meaningful to older females. There is no difference in needed PA amount between different genders in 85 year and older adults. VL - 12 IS - 3 ER -
St Joseph’s College of Nursing, University of Mount Saint Vincent, Riverdale, The United States
Elaine Marieb College of Nursing, University of Massachusetts Amherst, Amherst, The United States
Elaine Marieb College of Nursing, University of Massachusetts Amherst, Amherst, The United States
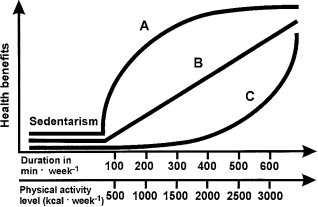
Figure 1. Schematic illustration depicting the relationships between PA level defined in minutes of participation per week or energy expended.
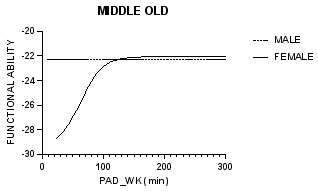
Figure 2. Functional ability and PA duration/week (min) in middle-old group.
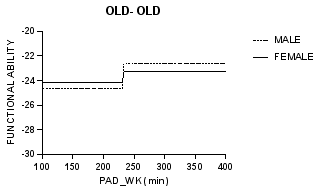
Figure 3. Functional ability and PA duration/ week in old-old group.
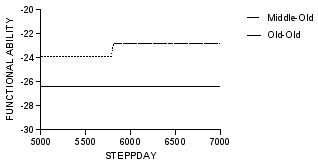
Figure 4. Relationship between functional ability and steps per day (STEPPDAY).
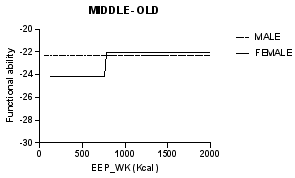
Figure 5. Functional ability and weekly energy expenditure (EEP_WK) in middle-old adults.

