Traditional auscultation remains diagnostically valuable but is limited by examiner subjectivity and access. Smartphone-based AI phonoscopy offers an opportunity for scalable self-screening for valvular heart disease. Stethophone®, an AI-enabled software as a medical device, was made available for download in Canada, the United States, and Ukraine. Users recorded heart sounds through the smartphone’s built-in microphones, processed and enhanced in real time using patented audio algorithms. Quality was automatically assessed, and users were prompted to re-record as needed. Recordings were analyzed for murmurs and aortic stenosis signatures using AI phonoscopy. Among 28,188 users producing 109,882 recordings, 91.7% of lay users and 89.0% of healthcare professionals achieved a clinically interpretable recording on the first attempt. Lay-users and healthcare professionals performed similarly (91% vs 89%). The most successful auscultation site was the tricuspid point; the left carotid least. Cardiac murmurs were detected in 16.3% of recordings, corresponding to 15.6% of users. Structural murmurs were identified in 7.0% of users (4.9% of recordings). Murmurs consistent with aortic stenosis were present in 6.3% of users. This study demonstrates that self-auscultation with a smartphone and dedicated medical software is highly feasible in lay populations, with quality results comparable to clinicians. Pathological murmurs, notably those of aortic stenosis, are common and highlight the potential for population-wide early detection of cardiac disorders.
| Published in | Science Journal of Public Health (Volume 14, Issue 1) |
| DOI | 10.11648/j.sjph.20261401.16 |
| Page(s) | 53-60 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Artificial Intelligence, Self-auscultation, Valvular Heart Disease, Aortic Stenosis, Digital health, Mass Screening
Role | 1st Attempt Success | 2nd Attempt Success |
|---|---|---|
Lay-Users | 91.7% | 91.1% |
Medical Professionals | 89.0% | 90.9% |
Recording point | Failed recordings (%) | |
|---|---|---|
7 | Left carotid | 16.7% |
8 | Right carotid | 10.9% |
1 | Erb’s | 7.7% |
3 | Apex | 7.2% |
4 | Pulmonary | 5.4% |
5 | Aortic | 5.0% |
6 | Erb’s right | 4.3% |
2 | Tricuspid | 3.4% |
Parameter | Total | w/Murmur | w/o Murmur | Innocent | Structural | with AS |
|---|---|---|---|---|---|---|
All subjects | ||||||
Number of cardiac recordings | 109882 | 17803 | 91579 | 12408 | 5395 | 4557 |
Percentage of total recordings | 100.0% | 16.3% | 83.7% | 11.3% | 4.9% | 4.2% |
Number of subjects | 28188 | 4388 | 14616 | 3533 | 1979 | 1786 |
Percentage of total subjects | 100% | 15.6% | 51.9% | 12.5% | 7% | 6.3% |
Medical professionals | ||||||
Number of cardiac recordings | 15003 | 3010 | 11993 | 1777 | 1233 | 874 |
Percentage of total recordings | 13.7% | 20% | 80% | 11% | 8.2% | 5.8% |
Number of subjects | 2219 | 497 | 1376 | 443 | 237 | 199 |
Percentage of total subjects | 7.9% | 22.4% | 62% | 20% | 10.7% | 9% |
Lay users | ||||||
Number of cardiac recordings | 94879 | 14793 | 79586 | 10631 | 4162 | 3683 |
Percentage of total recordings | 86.2% | 15.7% | 84.3% | 11.3% | 4.4% | 3.9% |
Number of subjects | 26196 | 3891 | 13240 | 3150 | 1560 | 1587 |
Percentage of total subjects | 92.9% | 14.9% | 50.5% | 12% | 6% | 6.1% |
AI | Artificial Intelligence |
AS | Aortic Stenosis |
CI | Confidence Interval |
PPV | Positive Predictive Value |
S1 | First Heart Sound |
S2 | Second Heart Sound |
TTE | Transthoracic Echocardiography |
VHD | Valvular Heart Disease |
| [1] | Nkomo, V. T., Gardin, J. M., Skelton, T. N., Gottdiener, J. S., Scott, C. G., Enriquez-Sarano, M. Burden of valvular heart diseases: a population-based study. The Lancet. 2006, 368(9540), 1005-1011. |
| [2] | Mangione, S. Cardiac auscultatory skills of physicians-in-training: a comparison of three English-speaking countries. The American Journal of Medicine. 2001, 110(3), 210-216. |
| [3] | Myerson, S., Prendergast, B., Gardezi, S., et al. GP auscultation for diagnosing valvular heart disease. Heart. 2017, 103(Suppl 3), A101-A102. |
| [4] |
U.S. Food and Drug Administration. 510(k) Premarket Notification: Stethophone (K231551). Available from:
https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm?ID=K231551 (accessed 9 February 2026). |
| [5] | Shortliffe, E. H., Sepúlveda, M. J. Clinical decision support in the era of artificial intelligence. JAMA. 2018, 320(21), 2199-2200. |
| [6] | Topol, E. J. High-performance medicine: the convergence of human and artificial intelligence. Nature Medicine. 2019, 25(1), 44-56. |
| [7] | Clifford, G. D., Behar, J., Li, Q., Rezek, I. Signal quality indices and data fusion for determining clinical acceptability of electrocardiograms. Physiological Measurement. 2012, 33(9), 1419-1433. |
| [8] | Vukanovic-Criley, J. M., Criley, S., Warde, C. M., et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Archives of Internal Medicine. 2006, 166(6), 610-616. |
| [9] | Finley, J. P., Sharratt, G. P., Nanton, M. A., Chen, R. P., Roy, D. L., Paterson, G. Auscultation of the heart: a trial of classroom teaching versus computer-based independent learning. Medical Education. 1998, 32(4), 357-361. |
| [10] | Tavel, M. E. Cardiac auscultation: a glorious past—and it does have a future! Circulation. 2006, 113(9), 1255-1259. |
| [11] | Watrous, R. L. Computer-aided auscultation of the heart: from anatomy and physiology to diagnostic decision support. In Proceedings of the 28th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 2006; pp. 140-143. |
| [12] | Constant, J. Bedside Cardiology. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999. |
| [13] | Lucas, J. W., Villarroel, M. A. Telemedicine use among adults: United States, 2021. NCHS Data Brief. 2022, (445), 1-8. |
| [14] | Patel, S. Y., Mehrotra, A., Huskamp, H. A., Uscher-Pines, L., Ganguli, I., Barnett, M. L. Trends in outpatient care delivery and telemedicine during the COVID-19 pandemic in the US. JAMA Internal Medicine. 2021, 181(3), 388-391. |
| [15] | Keesara, S., Jonas, A., Schulman, K. Covid-19 and health care’s digital revolution. The New England Journal of Medicine. 2020, 382(23), e82. |
| [16] | Rabbani, M. G., Alam, A., Prybutok, V. R. Digital health transformation through telemedicine (2020-2025): barriers, facilitators, and clinical outcomes—a systematic review and meta-analysis. Encyclopedia. 2025, 5(4), 206. |
| [17] | Inglis, S. C., Clark, R. A., Dierckx, R., Prieto-Merino, D., Cleland, J. G. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database of Systematic Reviews. 2015, (10), CD007228. |
| [18] | Estêvão, M. D., Fernandes, M. T., De Sousa-Coelho, A. L., Espírito-Santo, M., Nascimento, T. Telehealth for integrated cardiovascular and diabetes management: a scoping review. Journal of Diabetes Research. 2025, 2025, 1093671. |
| [19] | Liu, J. C., Cheng, C. Y., Cheng, T. H., Liu, C. N., Chen, J. J., Hao, W. R. Unveiling the potential: remote monitoring and telemedicine in shaping the future of heart failure management. Life. 2024, 14(8), 936. |
| [20] | Kuan, P. X., Chan, W. K., Fern Ying, D. K., et al. Efficacy of telemedicine for the management of cardiovascular disease: a systematic review and meta-analysis. The Lancet Digital Health. 2022, 4(9), e676-e691. |
| [21] | Kelly, C. J., Karthikesalingam, A., Suleyman, M., Corrado, G., King, D. Key challenges for delivering clinical impact with artificial intelligence. BMC Medicine. 2019, 17(1), 195. |
| [22] | Cabitza, F., Rasoini, R., Gensini, G. F. Unintended consequences of machine learning in medicine. JAMA. 2017, 318(6), 517-518. |
| [23] | Liu, X., Faes, L., Kale, A. U., et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. The Lancet Digital Health. 2019, 1(6), e271-e297. |
| [24] | Steinhubl, S. R., Muse, E. D., Topol, E. J. The emerging field of mobile health. Science Translational Medicine. 2015, 7(283), 283rv3. |
| [25] | Bhavnani, S. P., Parakh, K., Atreja, A., et al. 2017 roadmap for innovation—ACC health policy statement on healthcare transformation in the era of digital health, big data, and precision health. Journal of the American College of Cardiology. 2017, 70(21), 2696-2718. |
| [26] |
World Health Organization. Global Strategy on Digital Health 2020-2025. Available from:
https://www.who.int/publications/i/item/9789240020924 (accessed 9 February 2026). |
| [27] | Tromp, J., Jindal, D., Redfern, J., et al. World Heart Federation roadmap for digital health in cardiology. Global Heart. 2022, 17(1), 61. |
| [28] | Craig, W., Ohlmann, S. The benefits of using active remote patient management for enhanced heart failure outcomes in rural cardiology practice: single-site retrospective cohort study. Journal of Medical Internet Research. 2024, 26, e49710. |
APA Style
Opauszky, M., Ivanova, N., Shpak, Y., Marchenko, N. (2026). Population-Based Feasibility of AI-Enabled Self-Auscultation using Smartphones: Findings from 109,882 Recordings Across Three Countries. Science Journal of Public Health, 14(1), 53-60. https://doi.org/10.11648/j.sjph.20261401.16
ACS Style
Opauszky, M.; Ivanova, N.; Shpak, Y.; Marchenko, N. Population-Based Feasibility of AI-Enabled Self-Auscultation using Smartphones: Findings from 109,882 Recordings Across Three Countries. Sci. J. Public Health 2026, 14(1), 53-60. doi: 10.11648/j.sjph.20261401.16
AMA Style
Opauszky M, Ivanova N, Shpak Y, Marchenko N. Population-Based Feasibility of AI-Enabled Self-Auscultation using Smartphones: Findings from 109,882 Recordings Across Three Countries. Sci J Public Health. 2026;14(1):53-60. doi: 10.11648/j.sjph.20261401.16
@article{10.11648/j.sjph.20261401.16,
author = {Mark Opauszky and Nadia Ivanova and Yaroslav Shpak and Nataliya Marchenko},
title = {Population-Based Feasibility of AI-Enabled Self-Auscultation using Smartphones: Findings from 109,882 Recordings Across Three Countries},
journal = {Science Journal of Public Health},
volume = {14},
number = {1},
pages = {53-60},
doi = {10.11648/j.sjph.20261401.16},
url = {https://doi.org/10.11648/j.sjph.20261401.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20261401.16},
abstract = {Traditional auscultation remains diagnostically valuable but is limited by examiner subjectivity and access. Smartphone-based AI phonoscopy offers an opportunity for scalable self-screening for valvular heart disease. Stethophone®, an AI-enabled software as a medical device, was made available for download in Canada, the United States, and Ukraine. Users recorded heart sounds through the smartphone’s built-in microphones, processed and enhanced in real time using patented audio algorithms. Quality was automatically assessed, and users were prompted to re-record as needed. Recordings were analyzed for murmurs and aortic stenosis signatures using AI phonoscopy. Among 28,188 users producing 109,882 recordings, 91.7% of lay users and 89.0% of healthcare professionals achieved a clinically interpretable recording on the first attempt. Lay-users and healthcare professionals performed similarly (91% vs 89%). The most successful auscultation site was the tricuspid point; the left carotid least. Cardiac murmurs were detected in 16.3% of recordings, corresponding to 15.6% of users. Structural murmurs were identified in 7.0% of users (4.9% of recordings). Murmurs consistent with aortic stenosis were present in 6.3% of users. This study demonstrates that self-auscultation with a smartphone and dedicated medical software is highly feasible in lay populations, with quality results comparable to clinicians. Pathological murmurs, notably those of aortic stenosis, are common and highlight the potential for population-wide early detection of cardiac disorders.},
year = {2026}
}
TY - JOUR T1 - Population-Based Feasibility of AI-Enabled Self-Auscultation using Smartphones: Findings from 109,882 Recordings Across Three Countries AU - Mark Opauszky AU - Nadia Ivanova AU - Yaroslav Shpak AU - Nataliya Marchenko Y1 - 2026/02/27 PY - 2026 N1 - https://doi.org/10.11648/j.sjph.20261401.16 DO - 10.11648/j.sjph.20261401.16 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 53 EP - 60 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20261401.16 AB - Traditional auscultation remains diagnostically valuable but is limited by examiner subjectivity and access. Smartphone-based AI phonoscopy offers an opportunity for scalable self-screening for valvular heart disease. Stethophone®, an AI-enabled software as a medical device, was made available for download in Canada, the United States, and Ukraine. Users recorded heart sounds through the smartphone’s built-in microphones, processed and enhanced in real time using patented audio algorithms. Quality was automatically assessed, and users were prompted to re-record as needed. Recordings were analyzed for murmurs and aortic stenosis signatures using AI phonoscopy. Among 28,188 users producing 109,882 recordings, 91.7% of lay users and 89.0% of healthcare professionals achieved a clinically interpretable recording on the first attempt. Lay-users and healthcare professionals performed similarly (91% vs 89%). The most successful auscultation site was the tricuspid point; the left carotid least. Cardiac murmurs were detected in 16.3% of recordings, corresponding to 15.6% of users. Structural murmurs were identified in 7.0% of users (4.9% of recordings). Murmurs consistent with aortic stenosis were present in 6.3% of users. This study demonstrates that self-auscultation with a smartphone and dedicated medical software is highly feasible in lay populations, with quality results comparable to clinicians. Pathological murmurs, notably those of aortic stenosis, are common and highlight the potential for population-wide early detection of cardiac disorders. VL - 14 IS - 1 ER -
Department of Medical Science, Sparrow Acoustics Inc., St. John’s, Canada
Department of Medical Science, Sparrow Acoustics Inc., St. John’s, Canada
Department of Medical Science, Sparrow Acoustics Inc., St. John’s, Canada
Department of Medical Science, Sparrow Acoustics Inc., St. John’s, Canada
Figure 1.
Screenshots of social media materials presenting the Stethophone® application.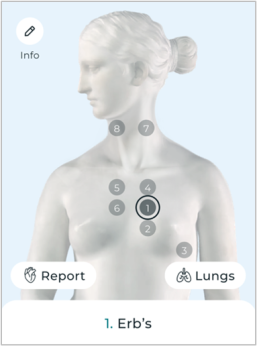
Figure 2. Locations of recording points used in the current research.

